Let’s talk about ligament injuries. Ligaments attach bone to bone and provide stability to a joint. An injury to the ligament is called a sprain. There are three grades of ligament injuries:
Grade I sprain is an injury to the substance of the ligament causing pain but minimal or no instability. (Instability means laxity or increased motion, which is not normal. The knee joint may feel as if it is giving out, if it is unstable, for example.)
Grade II sprain is a stretch injury to the ligament with a partial tear causing moderate instability.
Grade III sprain is a complete tear of the ligament and is associated with significant instability.
The medial collateral ligament of the knee (MCL) is the most common injury to a ligament around the knee. The medial collateral ligament and the lateral collateral ligament are most often injured by direct trauma such as an impact from the side (think football tackle here). The athlete will complain of swelling, pain, and instability on the inside (MCL) or outside of the knee (LCL).
Immediate treatment of ligament injuries is conservative including crutches and splinting. X-rays are required to rule out a fracture. Ongoing treatment usually includes functional hinge-brace. A hinged knee brace provides increased support and stability to the knee—more than an elastic brace or neoprene sleeve. The hinged brace is dynamic and allows movement so the knee does not get stiff.
Return to play after injury
An injured kid may return to play when there is no pain, when strength is equal to the uninjured side, and when the athlete is able to perform sport-specific activities (drills and skills associated with the sport) without pain.
Grade I sprains will usually take four to six weeks for the athlete to get back in the game. Grade II injury takes eight to ten weeks for full recovery, on average. Grade III injury takes about twelve to fourteen weeks to recover. Treatment of isolated MCL and LCL injuries do not require surgery. Conservative treatment of these ligament injuries is successful in most cases.
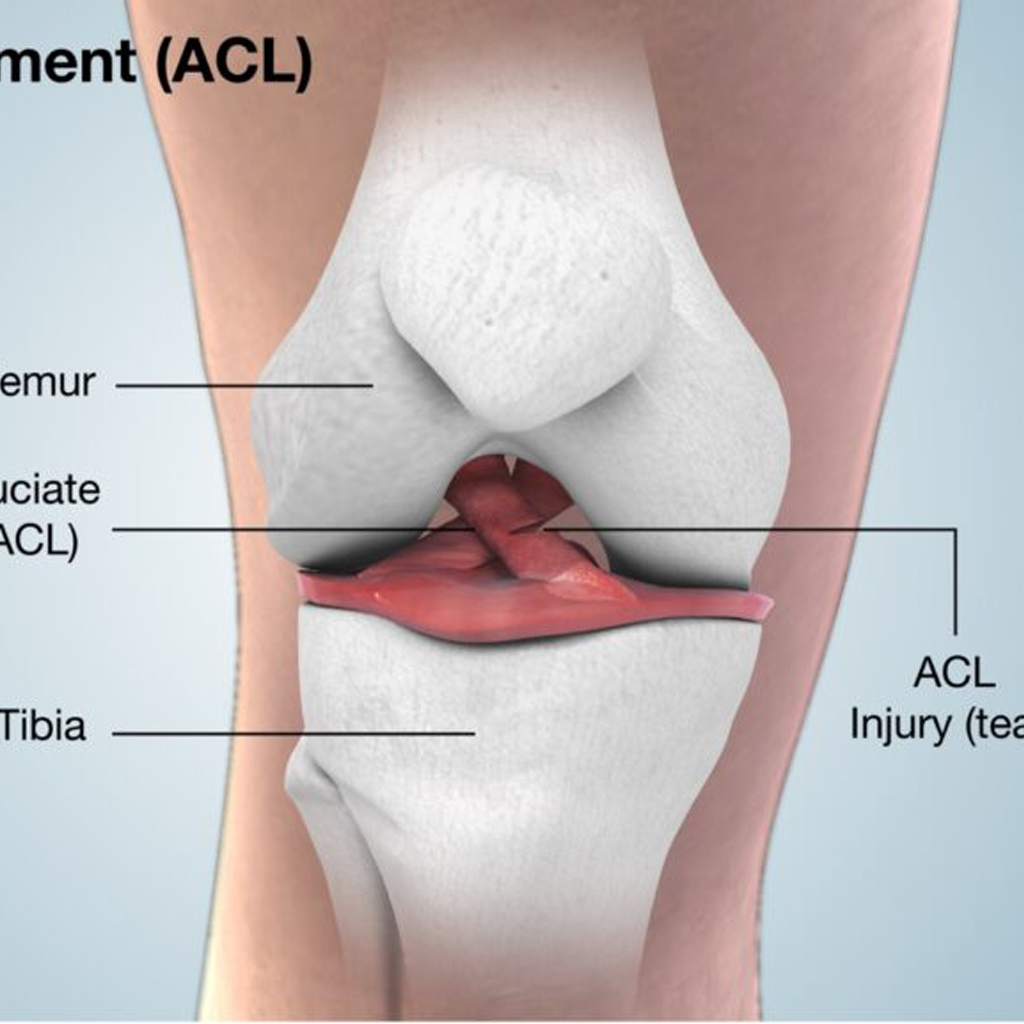
And then there’s the ACL. It has been said that the three most frightening letters in the NFL are A-C-L. An injury to this ligament is very serious. In the past, a tear of the ACL would have been career ending. Now it is considered season ending.
The anterior cruciate ligament helps stabilize the knee by connecting the tibia (shin bone) to the back part the femur (thigh bone). This connection of the two bones keeps the shin bone from sliding forward in relationship to the thigh bone. Usually, the ACL is a strong ligament and keeps the knee stable with cuts, twists, sudden stops, side-to-side motion, and pivoting.
In sports where there is stop-and-go activity such as basketball, tennis, football, and soccer, this ligament is a key stabilizer of the knee.

An injury to the ACL is much more common than to the PCL (posterior cruciate ligament) by about 10 to 1. The diagnosis of ligament injuries may be by history and physical examination. MRI can be used to reinforce the diagnosis.
If there is a minimal or partial tear of the ACL with only a little instability, the athlete can avoid surgery and go forward with rehabilitation. A brace must be used for a return to play in most sports. A complete tear of the ACL with significant instability will usually require surgery to repair the ligament in order for the young athlete to return to play.
The timing of surgery in the younger athlete is important because kids have open growth plates. Special testing (bone age) must be done to see how much growth is remaining in the bones.
If there is less than 1 cm of growth remaining, the athlete is treated as an adult. A reconstruction is recommended.
If there is more than 1 cm of growth remaining, ACL reconstruction may not be recommended. A modified technique may be suggested and discussed with the sports medicine doctor.
The most commonly used technique for ACL reconstruction in kids uses a technique that minimizes the risk of growth disturbance, and surgeons have developed techniques to avoid growth plate injury. We can delay reconstruction until maturity is complete but that might risk instability episodes and damage to the joint. I usually recommend reconstruction in order to reduce recurrent instability episodes and further damage to the joint.
ACL Reconstruction
An adult-type ACL reconstruction is usually done in females over age fifteen and males over sixteen. Otherwise, a graft is used to reconstruct the ACL and avoid hardware at the level of the growth plate. Any drill holes made to receive the graft should be small. With careful attention to surgical technique the ACL reconstruction in kids should be safe and effective.
If you are in this situation, talk with your surgeon and have him or her explain the options and the techniques. Ask questions about risk. Those are all fair points for discussion when it comes to ligament injuries.
Return to play after an ACL reconstruction is a minimum of six months. The initial period following ACL surgery (reconstruction) uses a brace and rehabilitation. The athlete will progress to full weight bearing, exercises, weight training, and sport-specific drills and skills. When the athlete returns to play, especially in a contact sport, a brace is usually recommended.
Although female athletes have been known to be at increased risk for ACL injury, there are studies that indicate that neuromuscular training may help prevent these ligament injuries. A study of female adolescent soccer players who participated in a fifteen-minute neuromuscular warm-up program twice a week showed they had a significant reduction in the rate of ACL injuries (Wilk et al., 1999).
This Swedish study looked at female soccer players who were twelve to seventeen years old. During the 2009 season, one group did the series of six warm-up exercises focused on knee control and core stability. One group did not do these warm-ups. The analysis of the data indicated a 64 percent reduction of ACL injuries in the group that did the neuromuscular warm-ups.
Most ACL Tears occur without direct contact
The message here is that knee exercises are recommended, especially for girls in sports. They just might have fewer knee injuries.
Most ACL tears occur without direct contact. The injury occurs during sports such as soccer, volleyball, basketball, football, gymnastics, and skiing. Usually the player will state that he or she planted a foot and pivoted sharply. Injury also occurs when the player locks or extends the knee after jumping and lands on a straight leg and not a flexed knee. The extended knee mechanism may be more common in girls.
ACL injuries can also happen when the athlete stops suddenly or is clipped or hit from the side with the foot planted. This is a painful injury, and the player knows something serious has happened in most circumstances. The athlete will feel that the knee gave way and may have felt or heard a pop.
One female volleyball player described the feeling as the worst pain she had ever felt, as she landed on an extended knee after a block. She felt as if everyone around her must have heard the pop, and she thought she had broken her leg as she fell to the ground and grabbed her painful knee. I cringe every time I see a girl land on an extended knee or run in an upright stiff position. They are just accidents waiting to happen.
ligament injuries
It is hard to walk on the leg after an ACL tear. The knee will get swollen in a couple of hours along with severe pain with weight bearing and bending of the knee. The first two days are usually the worst, so if surgery is required, it may be postponed until the swelling has decreased. At the same time an ACL tear occurs, it is not unusual for there to be an injury to the cartilage (meniscus) of the knee.
Teenagers are a high-risk group for ACL injuries
Teenagers are a high-risk group for ACL injuries. This may simply be because they are more active. The highest risk kids are those who play sports that involve cutting, pivoting, sudden stops and starts, and jumping.
Knee ligament injuries statistics for females are consistent across high school, college, and Olympic levels. Ankle and knee injuries, along with calf injuries, rank highest for injury severity and lost playing time in females. Females suffer more lower limb injuries while males suffer more facial injuries.
Females have a higher rate of serious knee injuries and are three to five times more likely to sustain an ACL injury when compared to males. Anatomical, hormonal, and biomechanical differences between females and males have been suggested as possible reasons why female athletes are more prone to sustain knee ligament injuries than male athletes.

Biomechanical testing of female basketball players, across all age groups, shows that the younger females tend to jump and land similar to boys until about puberty. The test was conducted by filming jumps off a plyometric box. The younger girls tend to land with their knees in alignment with their hips and ankles.
As the girls enter puberty, the knees start to fall into valgus (knock knees), placing more stress on the knee joint. This may be a result of the girls getting wider hips and attempting to keep their center of gravity and balance. It is very difficult to correct for this, even with rigorous training. However, strengthening the vastus medialis is a good exercise to help stabilize the knee in a female player. (The vastus medialis is the big muscle of the quadriceps on the inside of the thigh. Exercises such as squats and leg press on a machine can strengthen this muscle.)
Why Girls Get More ACL Injuries Than Boys
· Girls, more than boys, use the ligaments more than their muscles to stabilize joints in sports.
· Boys, at puberty, increase in height and develop lower leg muscle strength (and mass) at the same time, but girls don’t tend to develop lower extremity strength unless they strength train.
· Girls land with their legs in a more straight leg position (may be hip weakness) and cannot use their quadriceps muscles as shock absorbers as well as boys.
· Girls’ knees tend to go into valgus (knock knee) when they are landing from a jump, pivoting, and side-to-side movements, and this position does not provide as much balance.
· Girls have wider hips and this may contribute to the knee position of valgus (looks like they are caving in), as the body keeps the center of gravity going down the center of the body (plumb line), which puts more stress on the ACL.
· Boys use their hamstrings (back of thigh muscles) while jumping and girls generally use their quadriceps (front of thigh) muscles, which pulls the shin bone (tibia) forward and puts more stress on the ACL.
Now you know. Can an athlete, especially female athletes, do anything about the ACL vulnerability? Girls can’t change their anatomy, but they can strengthen their legs.
Leg strength is less in female athletes and they have slower muscle reaction times than males, which would increase the risk of injury. However, this is the one thing that can be corrected in females. Strengthen the muscles of the leg and the core muscles of the back, buttock, and abdomen, which keep the body upright.
Hamstrings help increase speed
The hamstrings need to be strong to keep the tibia in place during landings from jumps and sudden stops. In addition, the hamstrings help increase speed with which girls react to ACL stressing movements. If female athletes react slowly, they are unable to protect their ACL. Women need to strengthen their hamstrings to protect their ACL.
Plyometric exercises and instruction on proper jumping technique are also important to prevent injury. Good examples of these exercises are tuck jumps, squat jumps, 180-degree jumps, ankle bounce, and broad jump. Girls need to learn how to “stick” their landings and hold the landing point for five seconds. Girls should avoid landing on an extended knee (more common in females) and land with the knee flexed.